Is induction a good option for me?
Not many moms decide early in pregnancy that they want to start their labor with an induction. Often, the ones that do haven’t yet learned about all of their options. While educating themselves and making a plan for labor and birth, most of the parents I work with find that they want to avoid induction – especially pitocin. However, as that due date approaches and often *passes* (especially with first babies!), induction starts to look like an appealing option!
Going into week 39, 40, 41 and beyond, many moms begin feeling pressure to get things moving. Some of this pressure comes from their own discomfort and eagerness to be done with pregnancy and to hold their babies. Some comes from family, friends and even random strangers asking “When is that baby ever going to come?!?” And some of the pressure comes from care providers informing parents of the increasing risk to the baby as each day passes.
This is the trickiest part.
You know that you definitely don’t want to put your baby at risk! And if anything goes wrong, you need to have complete confidence that the decisions you made were the best possible decisions for your baby and yourself with the information that you had. So, what are these increased risks? And how do they compare to the risks of the induction itself?
As a doula, I have the induction conversation with nearly every single client. As a teacher, I talk about it in every class and training. It is a question that nearly every mother will face at some point toward the end of her pregnancy. Unfortunately, it is not a simple question! There are a lot of factors in making the decision whether or not to be induced. If you are facing this choice right now, let’s walk through some of the things you will need to consider in order to make a confident, informed decision.
Risks associated with going past your due date
It is true that the risks of something going wrong increase as a mother goes farther and farther past her due date.
Stillbirth
There is an increased risk of stillbirth from 39 to 42 weeks and beyond. As you can see in this graphic from Science and Sensibility, it is a surprisingly small increase, especially in mothers who are considered low-risk.
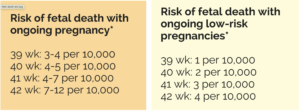
What I like about this graphic, is that you can see the incremental increase in risk. Going one day past your due date doesn’t suddenly triple your chances of losing your baby. This is true for the other risks we will discuss, as well.
Macrosomia
Macrosomia (babies larger than their gestational age) is often a concern that doctors will voice toward the end of pregnancy. The concerns with macrosomia include the baby getting “stuck” during delivery (which often includes the use of forceps, vacuum or c-section) and blood sugar concerns. However, going past a due date is only considered a contributing factor to macrosomia beyond 42 weeks. This condition is most commonly caused by diabetes that is not able to be controlled with medication, a mother who is significantly overweight or who gains an excessive amount of weight during her pregnancy. It is not commonly caused by going 1-2 weeks past due.
The longer the baby is in the uterus, the more likely it is that she will have a bowel movement. The risk of this happening in the amniotic fluid is that the baby may inhale it into her lungs which can cause serious breathing problems after birth. If meconium is found in the fluid after the water breaks, there will be pediatric nurses on hand when the baby is born to apply suction and remove any meconium from her airways.
Other risks
There is also an increased risk of low amniotic fluid, a higher chance of both infection and postpartum hemorrhage. Again, these risks increase incrementally with the greatest risks occurring after 42 weeks.
Do inductions lower c/s rates?
A study came out at the beginning of this year on elective inductions at 39 weeks called the ARRIVE Study. The buzz was that the results showed early, elective inductions lowered c-section rates. You can imagine the varied reactions! While there are many layers to this conversation, Rebecca Dekker of Evidence Based Birth has sifted through them for us and summarized it this way: If you are wanting a medical birth (as many mothers in this country do!), having an early induction can lower your c-section rate more than having a late induction. It may also leave you feeling more satisfied with your birth rather than having to wait.
However, the same satisfaction results are not going to be applicable to people wanting a natural or non-medical birth. Regardless of the desired type of birth, we need to hold up the results of this study against other methods of lowering c-section rates that have been found to have EVEN HIGHER success rates. These include: movement in labor, education during pregnancy, having a labor doula, laboring in water and using other comfort measures, having a supportive care provider and laboring in a stress-free environment. What we already know is that inductions bring about a higher cesarean rate when compared to those who labor with these other methods of support. For more detailed information on the ARRIVE study, see Rebecca’s facebook video where she walks through it step by step.
Risks associated with induction
There are certain risks with any method of induction. Any time we are trying to force someone’s body to do something it is not doing on its own, there is a chance that it won’t work as planned. This is true with both pharmaceuticals or natural methods.
Longer Labor
Whenever we try to force a body into labor before it is ready, it takes a bit longer. Unless the mother’s body was completely ready to go and we happened to nudge it at just the right time, induction births just take longer. This is true whether the induction is with pharmaceuticals or “natural” methods.
Increased Pain and Mental Stress
Many induction methods like cytotech, pitocin, and even nipple stimulation result in artificially strong, long and frequent contractions. This intense pattern also begins at earlier stages of labor than it would have on its own.
So, if an average first time mom has a 16 hour labor without interventions, she will usually spend half or more of that time in easily manageable, early labor at home. She might be working, eating, watching TV, taking naps, chatting with friends. With an induction, even if she labors for those same 16 hours, she will most likely have intense contractions for the entire labor. All of this will take place in a hospital room while watching the clock. As you can imagine, this leads to increased physical discomfort as well as increased mental stress.
Baby’s Heart Rate
Longer, stronger contractions early in labor is sometimes too much for babies to handle. Care providers and hospital staff will monitor the baby’s heart rate to see if he is responding well to the contractions. If he is not, they will try positioning the mother differently and will often back down on the pitocin (if it is being used) to see if the heart rate improves. If it continues to decline and delivery is not near, then a c-section is the result to ensure the baby’s safety.
Infection
Artificial rupture of membranes (breaking the water) is a non-medicinal induction method. The most common risk associated with this method is the significantly heightened risk of infection. Since the protective layer of the membranes is no longer intact, it is much easier for bacteria to enter. If the baby was still high or in a less-than-desirable position, breaking the water can also settle a baby’s head down into the pelvis in a funky way. This can prolong the length of the labor.
Extras
When a mother is induced at a hospital, there are some other things that come along with it. Most noticeably, she will need to be continuously monitored and must have an IV with fluids. Personally, these will have an impact on her freedom of movement and her stress level. Medically, the continuous monitoring is well known for false positives with regards to the the baby’s heart rate. This leads to an increase in further interventions and c-section. The IV fluids, if given over an extended period of time can cause edema (swelling) in both the mother and infant. This can have an impact on the baby’s weight and on breastfeeding.
The point
The point of this section is not to cause fear or to talk anyone out of an induction if they want one! The reason I have gone into detail about these risks is because care providers often do not discuss them in prenatal appointments. The risks of going past your due date may be the only ones that are talked about! In order to truly give informed consent for a procedure, you need to know the risks of doing it, AND the risks of not doing it, as well as any alternatives that may be available.
Failed Inductions
You have probably heard this term and may know someone this has happened to. A “failed induction” usually means that the mother’s body was not ready to go into labor. Sometimes the baby is not in a position to trigger the physical beginnings of labor. Sometimes the hormones that need to be released from the mother’s body, the baby’s body and the placenta have not reached the correct levels. Sometime the mother’s body has not yet constructed the receptor sites to receive the oxytocin hormone to begin labor. In that case, it doesn’t matter how much pitocin (synthetic oxytocin) she receives. Her body will not be able to utilize it. But how can you know these things before you go into the hospital to be induced??
There is a tool that care providers use to determine what the odds are of a successful induction. They determine how far the mother has already progressed on her own. The more she has progressed before an induction, the better indication that her body is already gearing up for labor. This method is the Bishop’s Score. You can see the 5 areas of progress to evaluate in the chart below. You will have to ask the doctor, midwife or nurse who does your cervical exam during your prenatal appointment for some of these details. They will always tell you your dilation and sometimes the effacement and consistency. The station and position you will most likely need to ask.
Bishop’s Score
| Cervical Exam | Points | |||
|---|---|---|---|---|
| 0 | 1 | 2 | 3 | |
| Dilation (cm) | ||||
| Effacement (%) | ||||
| Station | ||||
| Consistency | ||||
| Position | ||||
For each measurement, you add the associated points. For example, if you are 1cm dilated (1 point), 50% effaced (1 point), the baby is still high (0 points), your cervix feels soft (2 points) but is difficult for the doctor to reach (0 points), the final score would be 4 points. A score of 6 or less is not likely to lead to a successful induction. A score of 8 or above is “favorable” or much more likely to succeed.
Of course, this number is not going to guarantee your outcome in either direction. But it can be a valuable tool when deciding whether or not induction is a good choice for you and your baby.
Having the Conversation
There are many other unique factors in making the decision whether or not to induce. Your personal health history is a major consideration that you will need to discuss at length with your care provider. Women of size also have unique considerations. Jen McLellan has written an excellent blog post regarding obesity and stillbirth risks. There are definitely rare occasions in which the baby is safer on the outside than on the inside. However, going into these conversations with your care provider armed with the information in this post will put you many steps ahead in your conversation.
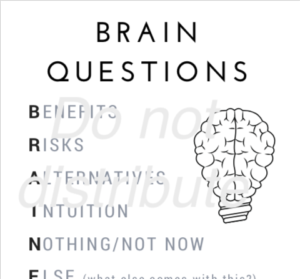
Remember to always ask your care provider about not only the risks of NOT inducing. Also ask about the risks associated WITH the induction. That way, you can balance the risks and benefits of each in a truly informed way. If you find it difficult to remember what questions to ask during appointments, consider using the BRAIN acronym. Click the image below to download the free printable PDF!
For information about other interventions – both medical and “natural” – as well as the opportunity to dive deeply into addressing anxiety, creating a birth plan and finding your way to calm and confidence, check out this $20 mini childbirth course: Birthing with Calm and Confidence.

Good luck with your planning and decision making for your birth! Remember ~ YOU know yourself and your body better than anyone else. You will make the best decisions for your baby!
References and Resources:
https://www.mayoclinic.org/healthy-lifestyle/pregnancy-week-by-week/in-depth/overdue-pregnancy/art-20048287
https://evidencebasedbirth.com/category/series/natural-labor-induction-series/
https://evidencebasedbirth.com/evidence-on-inducing-labor-for-going-past-your-due-date/
https://www.scienceandsensibility.org/blog/new-henci
https://clinicaltrials.gov/ct2/show/NCT01990612
http://perinatology.com/calculators/Bishop%20Score%20Calculator.htm